
You are reading one in a series of short posts translating the patient experience to an action-oriented context for clinicians.
My wheelchair was outfitted with a tray, which might be convenient if I were cruising the halls of the locked brain injury unit, snacking on Doritos I took away from lunch, sipping stale hospital coffee from a Styrofoam cup, with the red straw pinched on the end like the metal receiving mold of a stapler, greeting staff with a Cheshire grin—“should he be out of his room?” The tray, brittle plastic, sold to Boeing in the late-1970s to pop up from the arm rests. Ginger ale. Always ginger ale.
My tray was not for convenience, though, but for safety, my left-arm, limp with hemispatial neglect, a side-effect of a gross total resection, edema, and subdural fluid collection, which, for what it’s worth, is still there, in a pocket, inferior right parietal lobe, above the occipital lobe; though, my proprioceptive issues are greatly improved, no small thanks to the persistence, skill, and expertise of my therapy team, two OTs in particular, and my wife, who is, “his wife, not his therapist.”
The dead-fish left arm, kenesio-taped to the tray during early therapy sessions to keep it from getting caught up in the spokes of the wheelchair, had earned its independence. I was complicit in my in-room exercises, and for a reward, earned the activity of navigating my wheelchair without supervision around my room, to and from lunch, and down the hallway to my favorite reading spot, a large window at the end of the fourth floor, overlooking the main drive, a quarter mile or so, lined with trees, where I would read three Einstein papers during my stay. The staff likely is still not sure if I was actually reading Einstein, or, you know, “reading” Einstein.
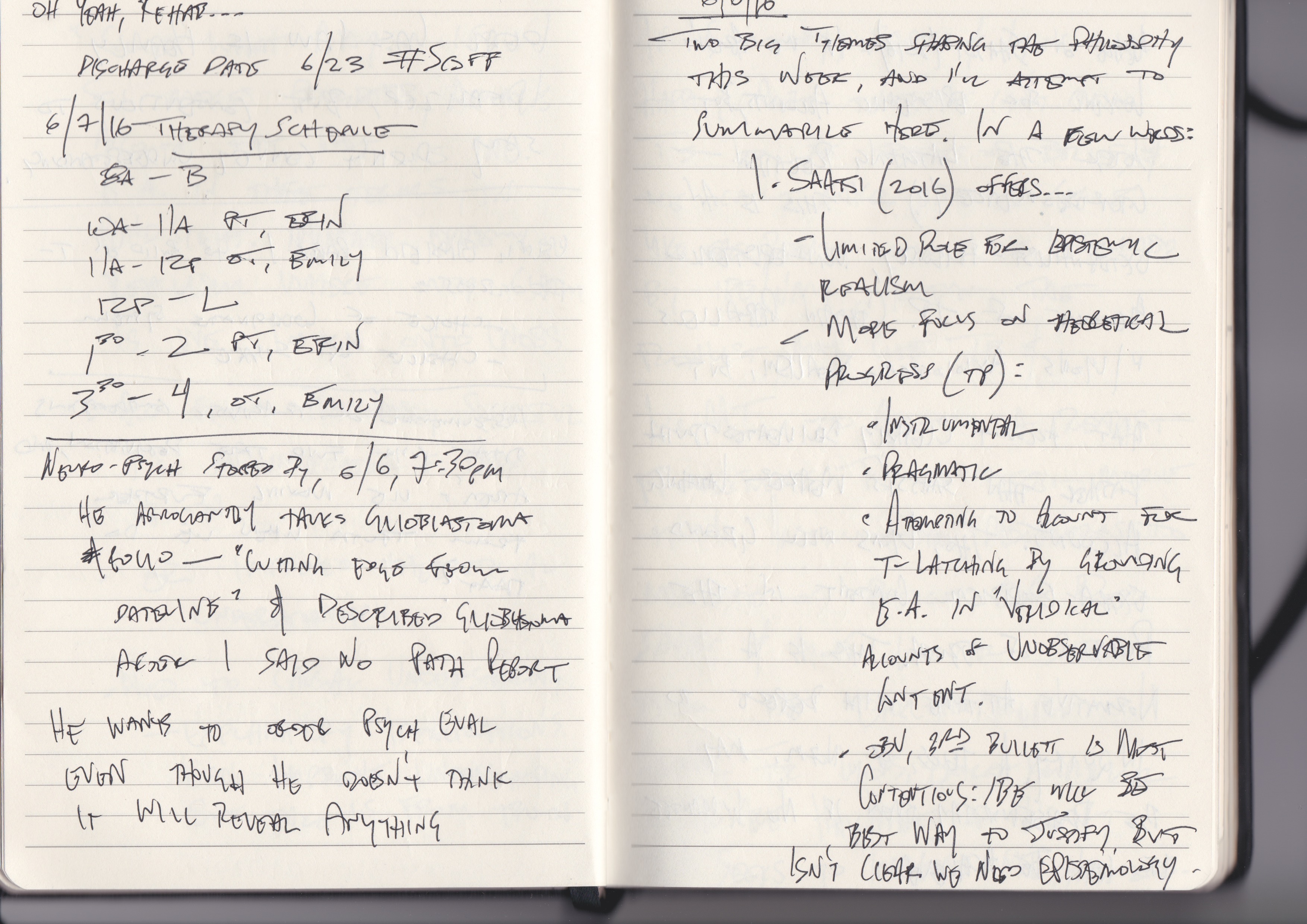
The neuropsychologist entered around 6:30pm, June 6, 2016—so says my journal, my reliable eyewitness to those few weeks. (A week and a half out from surgery.)
He pulled a chair to the center of the room.
Sat.
“You’ve been through a lot. How are you doing?”
“I’m really doing well, all things considered! I’m enjoying the schedule here, and I really appreciate the opportunity to rehab my motor and sensory deficits.”
This is my stock answer. I explain that I am expecting the pathology report soon to hear about the type of cancer that grew itself into a baseball-sized tumor in my right parietal lobe. “It will be good to know what we’re up against.”
I am still unsure if the pathology report was available in my records at that time, which the neuropsychologist would have, and probably should have, read, prior to his stop-and-chat, and it is not implausible to think everyone else had read it but was waiting for my neuro-oncologist to break the news. (Which would happen four days later on June 10, 2016.) Or maybe the neuropsychologist never read it. It is also possible that the pathology report was not yet available.
At any rate, my response, “…really waiting on that path report … can’t wait to hear what we’re up against,” is reason enough to suspect that this patient is unaware of his diagnosis.
“You appear to have a positive outlook. Do you feel anxious?”
[I’m in a locked brain trauma unit, separated from my family, less than two weeks out from major brain surgery, unsure of the type of brain cancer I have.]
“No, not anymore than what I would guess is to be expected. I actually feel pretty good, and I think having the mass resected from my brain has improved my overall health.”
[This much is accurate. My right ventricle was squashed into a pancake and the mass had occupied all available space in my parietal lobe, pinching the optic nerve bundle on its way back to the occipital lobe. I was having daily seizures, and episodic paralysis on my left side. Each of these symptoms improved after resection. I really was feeling pretty good post-op. Good enough to read Einstein, anyway.]
“Have you heard about the exciting new research for treating glioblastoma?” the neuropsychologist asks. He begins his ode to the polio vaccine: a soliloquy to research and the promise of a cure for glioblastoma. It is a grand love song to the miracles of modern medicine in which I tacitly feature as a supporting character.
In fact, this continues to be—the polio vaccine, I mean, a common response to people hearing about my diagnosis.
“Have you heard about this the polio vaccine!?”
It’s not just for New Deal Presidents, anymore.
This compulsion to share uplifting news grows from fascination and wonder with great respect and discomfort for our own mortality, “What if this were my diagnosis?” Our mortality is curious. It raises the Cartesian punch line that maybe I am strictly a thinking thing, and if that is the case, is that thinking separate from my body, or is it emergent from my physical processes? The churning, whirring, buzzing of a busy brain, and in the absence of these processes, so goes the thinking, and frighteningly enough, so goes me?
I think; therefore, I am.
I am not.
Therefore, I am not thinking.
The neuropsychologist continues.
“Mhmm,” I nod along.
“Have you watched the 60 Minutes Episode?”
“No, unfortunately I haven’t had the chance.”
“Maybe it was on Dateline. It’s really cutting edge.”
I rally from somewhere deep, “Oh! Thanks so much for sharing the information!”
Let us not give ourselves over to cynicism, it fails to be productive, but neither should we fail to learn lessons when available. My talented and bright sister-in-law would call this a #teachablemoment. I advocate a person-centered approach to healthcare, and I gather many of you do, too, if only implicitly. What I mean is this: there is a time in medicine’s recent past that, owing to any number of factors, the piss-poor antiseptic practices, the intimidation of meddling with one’s personal constitution, the inaccessibility of information, or maybe the poor track record of doctors was still appreciably better than at-home treatment, a patient would visit a doctor when sick, take his advice—certainly a “he” in these cases, and bite the bullet, drink the booze, what doc says, goes. If you’re not that sick, you don’t need the doctor, anyway, and if you’ve called for the doc, I suspect his advice ought to be followed.
The doctor-patient relationship I mean to evoke in this instance brings to mind fond cultural memories of our Little House on the Prairie obsession with frontier America, unbridled horses, one-room schoolhouses, and whatever else they packed into Back to the Future III. The doctor was an authority. An expert. An altruistic one at that, and so, what reason would we have not to take doc’s prescription to heart?
The following is my thesis. Our doctors do their best work when their patients are active, involved, engaged, participatory, willing, and honest. A person-centered (or “patient-centered,” if you like, but that sees the person as patient first, like the difference between “a colored person” or a “person of color,” yes?), anyway, a person-centered approach to healthcare places a responsibility on the person seeking treatment to view their self as an advocate, as vitally important to healing, as a part of their medical team. Doctors who are committed to person-centered healthcare inspire and recognize these qualities in the persons under their care.
Consider these mistakes committed by the doctor who visited me that evening: my diagnosis was unknown to me at the time of our meeting. Was I told my diagnosis during that conversation? I cannot answer that question.
The polio vaccine is administered for treatment of GBM under certain conditions to patients who meet strict qualification guidelines for acceptance into a specific research trial. Was application to that research trial recommended to me during that conversation? I cannot answer that question.
Dateline is not cutting edge; a recent peer-reviewed journal article in a field of specialty is. Was I provided with the resources to learn more about this new treatment option during that conversation? I was not.
Doctor exits.
I scribble away in my notebook. I breathe deeply. I position my tired left arm, using my able right arm, onto the wheel, and push myself to the wardrobe in my small hospital room to begin changing for bed. The path is obstructed. Doctor has left his chair in the center of the room.
Each of these transactions during this experience—the diagnosis, the clinical research, moving the chair, I was not empowered to take an active role in my own care; it was about doctor as authority, doctor as expert, and that is why this experience, despite all my rattled, broken, and fatigued body has been through these few months, stands out as one of the most negative. Power was withheld from me that evening.
Soon, or in some time, we will visit a sick friend; maybe a dying friend, and this will be an opportunity to empower or to hold on to power. I ask that we embrace the former and recognize when we are stubbornly adhering to the latter for our own insecurities, fears, or discomfort.
Keep learning. Keep fighting.
Cheers- AH

Leave a comment